Healthcare has spent decades optimising itself around scale.
We standardised pathways, digitised workflows, normalised data models, and built systems designed to treat populations efficiently rather than individuals uniquely. This made sense: health systems needed to be safe, repeatable, auditable, and financially sustainable. Digital health followed suit with generic platforms, standard codes, common denominators.
Yet we now find ourselves at a crossroads.
With advances in genetics, gene editing technologies such as CRISPR, and the growing feasibility of patient-specific drugs and therapies, healthcare is moving rapidly toward genuinely personalised treatment. The science is becoming patient-centred at a molecular level, however but our systems are not.
This is the paradox of modern healthcare.
Personalised Medicine vs Generalised Systems
The concept of patient-centred care is not new. What is new is the scale at which personalisation is becoming possible.
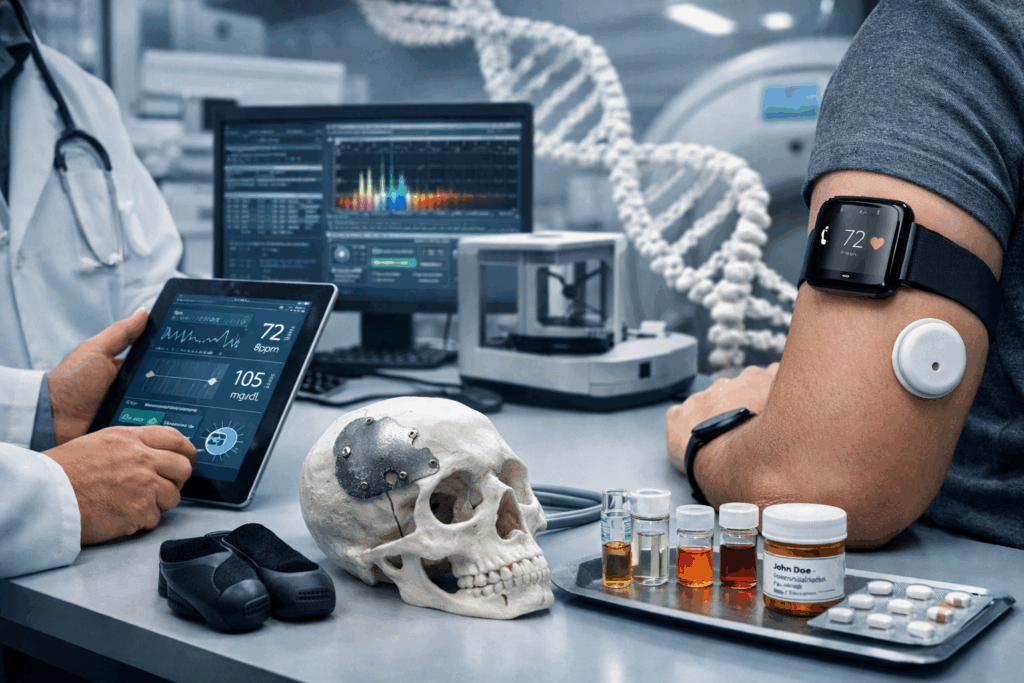
Genomics, pharmacogenetics, AI-assisted diagnostics, and adaptive therapies all point toward treatments tailored to the individual rather than the average. At the same time, patient wearables, with heart rate monitors, glucose sensors, activity trackers, sleep devices; that are generating continuous, patient-specific data streams that reflect how individuals actually live, transverse their journey, and hopefully respond to treatment.
Yet most digital health strategies have historically aimed to do the opposite: remove variation.
We built systems that:
- Standardise clinical workflows
- Abstract patients into datasets
- Optimise for interoperability, not individuality
- Reward conformity to pathways rather than deviation from them
Wearables now challenge this model. They introduce longitudinal, contextual, and highly individual data into systems that were designed for episodic, standardised snapshots of care.
A Teaching Moment: Where the Theory Breaks
Last year, while lecturing students on personalised care technologies, a recurring challenge emerged. Students struggled with the principles, not because they lacked understanding, but because the ideas directly contradicted current digital health strategies.
The contradiction was clear:
- We teach personalised care
- We build generic systems
Patient wearables became a particularly powerful example. Often categorised under clinical engineering or digital health, wearables promise personalised monitoring and early intervention; yet they are frequently forced into rigid data models or sidelined as “non-clinical” because they do not fit existing workflows. Often utilising frameworks, to purchase a one-size fits all for the entire organisation; with disregard for thorough requirements gathering from potential service clients the variation and gaps are never discovered.
To bridge this gap, we turned to rehabilitation engineering as a case study.
What Rehabilitation Engineering Gets Right
Rehabilitation engineering has, by necessity, always been patient-specific.
No two patients are the same. No two outcomes are identical. No two solutions can be easily templated.
Rehabilitation services routinely integrate bespoke devices, adaptive technologies, and increasingly, patient wearables; that tuned not just to diagnosis, but to lifestyle, environment, and functional goals. The design processes, audit and regulation compliance are capable of understanding the uniqueness of the patient and making it the focus of the design.
Similarly, specialties such as maxillofacial surgery operate in domains where each case is anatomically, functionally, and clinically unique. These departments have long embraced:
- Individualised assessment (Discovery)
- Outcome-focused design (Define)
- Iterative, patient-specific solutions (Develop)
- Continuous monitoring of outcomes (Deliver)
They did not scale by removing variation, they scaled by managing it.
The Real Question
The question is not whether personalised medicine is coming, it already is.
The real question is this:
After years of building systems that deliberately removed patient uniqueness, how will health services adapt to an era that demands patient-centred treatment models?
Are our electronic health records capable of supporting patient-specific therapies and continuous wearable data rather than categorising them? Can clinical engineering and digital teams work together to govern, validate, and integrate wearables at scale? Will procurement, regulation, and governace models cope with treatments and technologies that don’t fit standard pathways?
Looking Forward
Patient-centred healthcare cannot simply be layered on top of existing digital infrastructure. Wearables, like personalised therapies, expose the limitations of systems built for uniformity.
If healthcare is to truly embrace personalised treatment, it may need to rethink:
- How patient-generated data is classified and trusted (TRE)
- How clinical engineering and digital functions collaborate
- How outcomes are defined beyond traditional clinical encounters
Ironically, the future of healthcare may depend on relearning lessons already embedded in parts of the system that never forgot the patient as an individual.
The question now is whether the rest of healthcare is ready to catch up.